Pataday | United States
This site is available in English
Pollen Levels, Weather & Air Quality Forecast
Eye Allergens Are Out There.
Eye Allergy Itch Relief Is Here.

Knock Out Your Itchy Allergy Eyes
#1 Selling Eye Allergy Itch Relief Brand¹
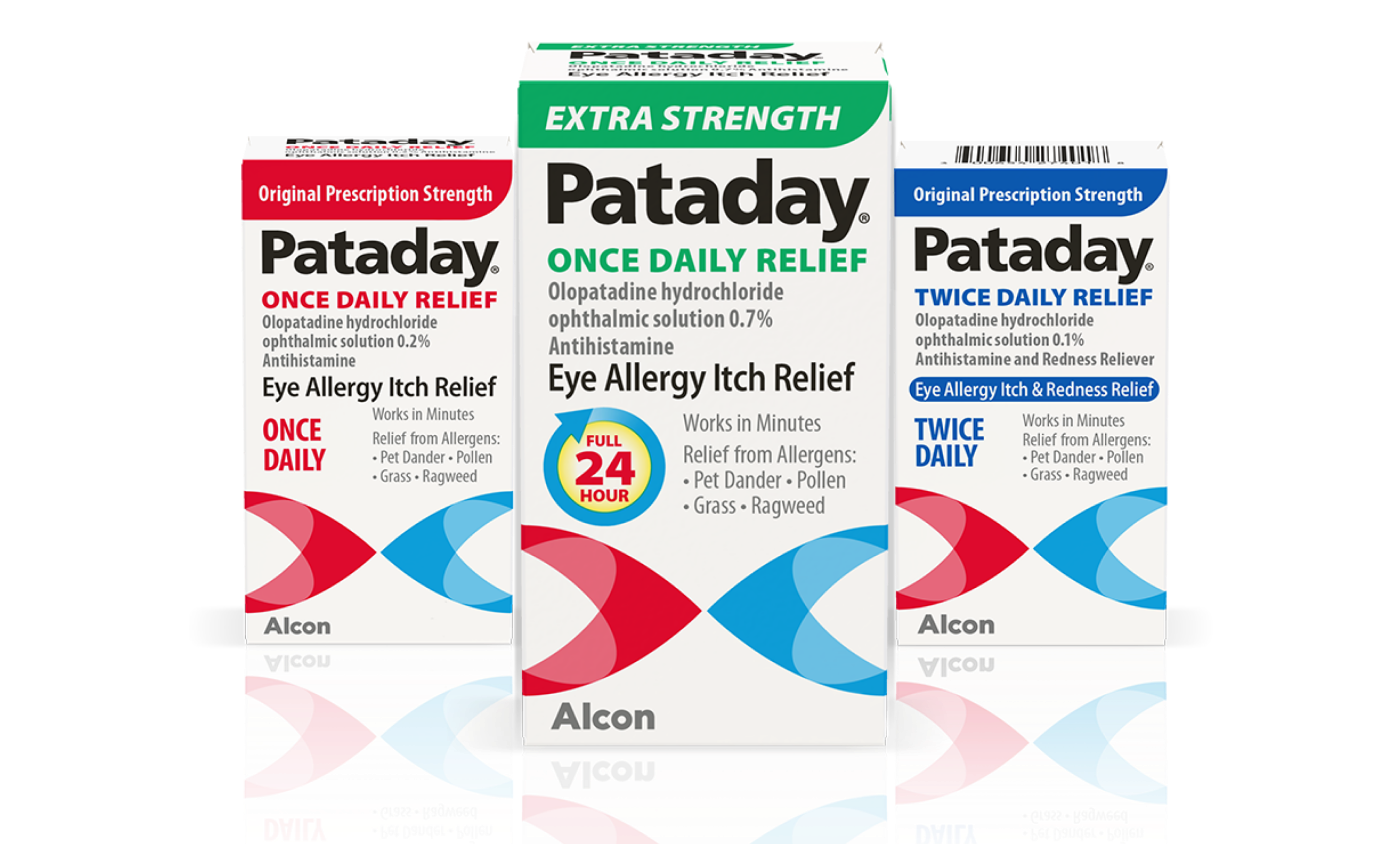
Find the Pataday That’s Right for You
Save with a Pataday Coupon
Register through MyAlcon for Pataday coupons and information on our trusted eye care products.
Save with a Pataday Coupon
Register through MyAlcon for Pataday coupons and information on our trusted eye care products.


You’ll Love Pataday
**Offer valid through 12/31/25. Receipt required. For full terms & conditions, click button above. Void where prohibited.
*TERMS AND CONDITIONS. Satisfaction guarantee available only for Pataday Eye Allergy Itch Relief products purchased between 1/1/24 and 12/31/25 U.S. Central Time. To request a refund, fill in the form at rapid-rebates.com/pataday and upload the receipt for your purchase. An eligible purchaser will receive a refund of the price actually paid for the product by the purchaser; this excludes the amount of any coupon or other discount applied at the time of purchase. Requests must be received by 5:00 p.m. U.S. Central Time on 1/31/25. Offer is void where taxed, restricted, or prohibited. Allow 8 to 10 weeks after submission for eligibility confirmation and delivery of your check. Limit one (1) refund per address. Alcon Vision, LLC reserves the right to confirm the identity of any purchaser.
Have Questions About Pataday?
Follow Us on Social Media
References:
1. Circana Eyecare Allergy MULO + AMZN 1P/3P, L52 WE 01-28-24